Some users may experience temporary issues accessing parts of the site. Thanks for your patience.
- Office Hours Mon - Fri 9:00 am – 4:00 pm EST
Dr. Richard Roblee is an airway-focused orthodontist that practices in Fayetteville, AR. Dr. Roblee is one of our featured speakers at the 2020 International Airway Symposium. He is also the author of Interdisciplinary Dentofacial Therapy: A comprehensive Approach to Optimal Patient Care. Kelley Richardson, our Airway Curriculum Liaison, sat down with him to discuss his interdisciplinary approach and how Dr. Peter Dawson helped shape his overall philosophy.
Kelley: When you spoke at the American Association of Orthodontists (AAO) meeting about digital smile design, how much was related to your airway patients versus digital dentistry?
 Dr. Roblee: I’ve found if I made it about airway, the turnout may not have been as strong. I think when it comes to airway, if you’re not part of the solution, you’re part of the problem. I think everybody needs to at least have a basic knowledge of airway problems. Whether they are going to treat or not, they need to recognize it and get somebody who can treat it. It is about overall philosophy. The exciting thing for me is that Dr. Pete Dawson is an important part of my upbringing, just like thousands and thousands of other dentists. Pete actually wrote the foreword to my textbook on interdisciplinary dentistry. He taught me to have certain basic principles that I’m not going to violate. The goal is to continue to produce excellent results in all the different facets of dentistry but it’s also to motivate patients to let you do the things that you need to do as a health professional. I have found that most of my airway patients don’t initially come in for airway. They don’t know they have airway problems. My philosophy is every patient is an airway patient until proven innocent, and that’s important.
Dr. Roblee: I’ve found if I made it about airway, the turnout may not have been as strong. I think when it comes to airway, if you’re not part of the solution, you’re part of the problem. I think everybody needs to at least have a basic knowledge of airway problems. Whether they are going to treat or not, they need to recognize it and get somebody who can treat it. It is about overall philosophy. The exciting thing for me is that Dr. Pete Dawson is an important part of my upbringing, just like thousands and thousands of other dentists. Pete actually wrote the foreword to my textbook on interdisciplinary dentistry. He taught me to have certain basic principles that I’m not going to violate. The goal is to continue to produce excellent results in all the different facets of dentistry but it’s also to motivate patients to let you do the things that you need to do as a health professional. I have found that most of my airway patients don’t initially come in for airway. They don’t know they have airway problems. My philosophy is every patient is an airway patient until proven innocent, and that’s important.
Pete taught me very early on to treat comprehensibly. With a foundation of airway, who else in healthcare can treat major underlying health issues and make people more beautiful at the same time? That’s us, and it is special. We’re talking about people that have:

With medications like:
What’s going on is they have been treated all of their life by symptoms, not by what’s really going on underneath. I think this is where dentistry is on the frontline.
I’m known for treating extremely complex problems. When you start learning more, you start wondering why don’t we start preventing these issues and treating them earlier on? That is where I take a mixed approach starting at birth. Look at anthropological events that are published in anthropology literature. See Origins of Dental Crowding and Malocclusion: An Anthropological Perspective by Jerome Rose, PhD and Dr. Richard Roblee, Compendium 2009. It’s amazing how after each generation, we are getting smaller and smaller. Meaning we are getting smaller arches, and that is why in the past we’ve had to take out a lot of teeth. I am a firm believer that taking out teeth does not cause airway problems. However, when you take out teeth, you are treating to the small jaws, and you’re not diagnosing the most important problem and that is the airway. The airway is all about volume. The oral cavity and the nasal cavity are the gateway to overall health. The airway has to be conducive with:
Kelley: How are you able to create more oral cavity volume in an adult patient? Are you able to move an adult maxilla forward non-surgically?
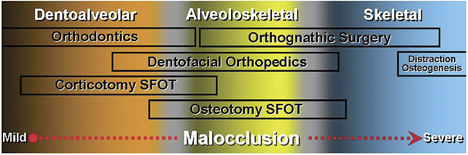
Dr. Roblee: That’s a little bit more complicated. What we’re doing is we’re creating a bigger box. We’re not moving the skeletal per se. We are creating significantly more volume and we break things down into the clinical components. During the Airway Symposium, I will talk about this in my presentation. But typically, we look at skeletal problems, and then we look at dentoalveolar problems. Dentoalveolar problems position the teeth in the bone. The skeletal or the overall base of the dentoalveolar complex. We treat something that I’ve coined alveoloskeletal problems. That’s the relationship of the dentoalveolar foundation to the skeletal base. A lot of these problems aren’t necessarily skeletal problems but that the alveolar complex has collapsed, and a lot of that is through lifelong malfunction of the soft tissue.
Kelley: Are you saying that you could dentally upright the teeth to put them back into the alveolar complex and treat a patient with myofunctional therapy, and that will solve a lot of problems?
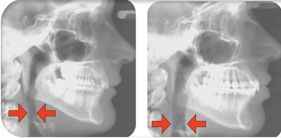
 Dr. Roblee: Yes. We change the relationship of the dentoalveolar complex to the skeletal base through clear aligners and surgically facilitated orthodontic treatment (SFOT), which is a minor gum surgery and less invasive than having wisdom teeth taken out. After that, we combine that with myofunctional therapy. Myofunctional therapy is critically important because what you have to remember is the lower face and the dental alveolar complex doesn’t form. It’s formed by soft tissue function, that is why they got there to begin with. If you don’t address that, it’s not going to be stable and you’re going to have continued long-term problems. We go through a very scientific, medically-based, work-up, and analysis and treatment to get them to where you think that this is going to help them.
Dr. Roblee: Yes. We change the relationship of the dentoalveolar complex to the skeletal base through clear aligners and surgically facilitated orthodontic treatment (SFOT), which is a minor gum surgery and less invasive than having wisdom teeth taken out. After that, we combine that with myofunctional therapy. Myofunctional therapy is critically important because what you have to remember is the lower face and the dental alveolar complex doesn’t form. It’s formed by soft tissue function, that is why they got there to begin with. If you don’t address that, it’s not going to be stable and you’re going to have continued long-term problems. We go through a very scientific, medically-based, work-up, and analysis and treatment to get them to where you think that this is going to help them.
Kelley: On the topic of a medically-based approach, who are the healthcare professionals that make up your interdisciplinary team?
Dr. Roblee: We actually have two myofunctional therapists in the office. One is a hygienist, a myofunctional therapist, and lactationist, because it starts at birth. I have another myofunctional therapist who’s really outstanding with the young children, teaching them, educating them. It’s not just general myofunctional therapy.
Outside of that we really work closely with:
I think it’s absolutely critical we work with our medical counterparts. That I can’t say that enough. We don’t want to be messing around if there is something more important going on that we don’t have the capacity to properly diagnose. But the hardest part with getting your team together, is the fact that you have to get the medical people on board, and sometimes that’s difficult. We, as dentists, can help them. I think the most important thing for somebody who wants to jump into this is try to get the best education you can and understand it from a more generic perspective.
This is part 1 of a 2-part interview. Stay tuned for part 2 coming next month.
ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry.
Concerns or complaints about a CE provider may be directed to the provider or to the Commission for Continuing Education Provider Recognition at ADA.org/CERP.

